It is DISH don’t confuse with AS Or OA spine
DISH stands for diffuse idiopathic skeletal hyperostosis.
DISH is known as Forestier’s disease as this condition was described by Forestier and Rotes-Querol over 50 years ago. It was termed was termed senile ankylosing hyperostosis.
Epidemiology (discussion of USA stats only):
1. DISH is very common, affecting between six and 12 percent of North Americans.
2. It rarely occurs among people younger than 50.
3. It affects more men than women.
DISH is thought to be the second most common form of arthritis after osteoarthritis. It affects between six and 12 percent of North Americans, almost always occurring among people older than 50. Unlike most types of arthritis, DISH occurs more often among men (65%) than women (35 %), and affects 28 percent of men over the age of 80.
What signs & symptoms may the patients present with:
1. Back pain and stiffness, especially in the middle area of the back
2. Sharp pain associated with bending or twisting of the back
3. Problems with swallowing and neck movement
4. What seems like “tendonitis” in the shoulder, elbow, knee or ankle.
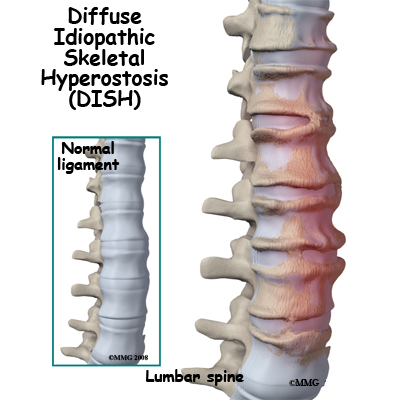
5. DISH is characterized by excessive bone growth along the sides of the vertebrae of the spine
6. It also involves inflammation and bone growth where tendons and ligaments attach to bone, such as at the elbow, knee and the heel of the foot.
Discussion:
In the absence of validated diagnostic criteria the diagnosis is usually based on the definition suggested by Resnick and Niwayama. This radiographic approach requires the presence of right-sided, flowing, coarse osteophytes in the thoracic spine, connecting at least four contiguous vertebrae, or ossification of the anterior longitudinal ligament, preserved intervertebral disk height in the involved segment, and the absence of apophyseal joint ankylosis and sacroiliac joint involvement.
According to Colina M et al, as seen on radiographic images D.I.S.H. presents characteristically with hyperostosis of the antero-lateral aspect of the spinal column, that sometimes leads to bone ankylosis, and by ossification of extra-spinal entheses. Other features include:
1. Ossification of the ALL (anterior longitudinal ligament) of the spine causes the formation of flowing osteophytes, while intervertebral disc space is quite preserved in early phases of the disease.
2. Pain and stiffness in spine usually worsened by inaction and dampness.
3. Appendicular skeleton is symmetrically involved in early phases of the disease. Most affected sites are being feet (planter fascia), olecranon and patella. Hip involvement is also frequent and may lead to severe disability and represents an important cause of invalidity.
Association with other diseases: The pathogenesis is not fully understood, but several factors have been implicated in the disease based on frequent associations with various metabolic conditions. Some of these factors are: hyper-insulinemia with or without diabetes mellitus, obesity, gout, dyslipidemia, and prolonged use of isoretinol.
1. This condition is often associated with the metabolic derangement of type 2 diabetes.
2. Primary hypertension, its cardiovascular aftereffects and lithiasis are also often present in these patients.
3. PLL (posterior longitudinal ligament) may lead to serious repercussions on the spinal cord & root anatomies & functions. Medullary canal stenosis may present with myelopathic features; presenting features are indicative of site of such changes.
Differentiating features between DISH & AS are:
The inflammatory spondyloarthropathies are usually easily distinguishable from non-inflammatory conditions. The clinical history, physical examination, extra-articular features, laboratory results, and various imaging modalities help in reaching the correct diagnosis. Kozanoglu E & colleagues and Moreno AC & colleagues reported Simultaneous occurrence of diffuse idiopathic skeletal hyperostosis and ankylosing spondylitis. However the following features are of importance:
1. HLA B27
2. Spinal fracture is well known in ankylosing spondylitis but exceptional in diffuse idiopathic skeletal hyperostosis (2).
3. SI joint involvement & it’s radiological features are of paramount importance in diagnosis of AS. According to Maertens M et al CT scan is helpful in differentiating the sacroiliitis of spondylarthropathies (6). However Computed tomography of the sacroiliac joints revealed several abnormalities including asymmetric intraarticular partial fusion, osteophytes with or without bridging, and vacuum phenomenon (5). According to Maertens M et al radiological differentiating points are:
a. absence of left side ossified enthesis (it is said that becuaes of presence of big abdominal vessels on left side this side enthesis are not ossified) & osteophytes.
b. The predominantly horizontal nature of the enthesiophyte in DISH.
c. A midthoracic notch was described in DISH which seemed to be confined to noninflammatory conditions, but is not found in ankylosing spondylitis.
Peculiarity of Radiological features of fractures in both AS & DISH (2)
1. Spinal fractures in patients with ankylosing spondylitis or diffuse idiopathic skeletal hyperostosis generally occur spontaneously or after low-energy trauma. Subsequent complications have serious consequences. Late diagnosis either results from missing a radiologically visible fracture or from the presence of an occult "paper thin" fracture.
2. Repeating standard x-rays the second and third weeks and use of a spiral scan or multiple spiral scan could provide early diagnosis.
Physiotherapy in DISH:
Physiotherapy in DISH is individualized according to the presentation. Spinal presentations are treated with mobilization for pain reduction. It must be noted though DISH mostly affects thoracic area, lumbar & cervical area pain may be presented by the patients. Strength training low load high repetition exercises. For acral enthesiopathies electro-therapeutics, soft tissue therapies, mobilization and strengthening can go side by side. Promotion of proper physical activity & modification of stressful ones are also key to successful management. Hydrotherapy is also a useful tool.
References: 1. Reumatismo. 2006 Apr-Jun;58(2):104-11. 2. Rev Chir Orthop Reparatrice Appar Mot. 2004 Sep;90(5):456-65. 3. Rev Rhum Engl Ed. 1996 Apr;63(4):292-5. 4. Clin Rheumatol. 2002 Jun;21(3):258-60. 5. J Rheumatol. 1988 Oct;15(10):1506-11. 6. Clin Rheumatol. 1992 Dec;11(4):551-7. 7. http://www.ima.org.il/imaj/ar03jul-11.pdf.
Epidemiology (discussion of USA stats only):
1. DISH is very common, affecting between six and 12 percent of North Americans.
2. It rarely occurs among people younger than 50.
3. It affects more men than women.
DISH is thought to be the second most common form of arthritis after osteoarthritis. It affects between six and 12 percent of North Americans, almost always occurring among people older than 50. Unlike most types of arthritis, DISH occurs more often among men (65%) than women (35 %), and affects 28 percent of men over the age of 80.
What signs & symptoms may the patients present with:
1. Back pain and stiffness, especially in the middle area of the back
2. Sharp pain associated with bending or twisting of the back
3. Problems with swallowing and neck movement
4. What seems like “tendonitis” in the shoulder, elbow, knee or ankle.
5. DISH is characterized by excessive bone growth along the sides of the vertebrae of the spine
6. It also involves inflammation and bone growth where tendons and ligaments attach to bone, such as at the elbow, knee and the heel of the foot.
Discussion:
In the absence of validated diagnostic criteria the diagnosis is usually based on the definition suggested by Resnick and Niwayama. This radiographic approach requires the presence of right-sided, flowing, coarse osteophytes in the thoracic spine, connecting at least four contiguous vertebrae, or ossification of the anterior longitudinal ligament, preserved intervertebral disk height in the involved segment, and the absence of apophyseal joint ankylosis and sacroiliac joint involvement.
According to Colina M et al, as seen on radiographic images D.I.S.H. presents characteristically with hyperostosis of the antero-lateral aspect of the spinal column, that sometimes leads to bone ankylosis, and by ossification of extra-spinal entheses. Other features include:
1. Ossification of the ALL (anterior longitudinal ligament) of the spine causes the formation of flowing osteophytes, while intervertebral disc space is quite preserved in early phases of the disease.
2. Pain and stiffness in spine usually worsened by inaction and dampness.
3. Appendicular skeleton is symmetrically involved in early phases of the disease. Most affected sites are being feet (planter fascia), olecranon and patella. Hip involvement is also frequent and may lead to severe disability and represents an important cause of invalidity.
Association with other diseases: The pathogenesis is not fully understood, but several factors have been implicated in the disease based on frequent associations with various metabolic conditions. Some of these factors are: hyper-insulinemia with or without diabetes mellitus, obesity, gout, dyslipidemia, and prolonged use of isoretinol.
1. This condition is often associated with the metabolic derangement of type 2 diabetes.
2. Primary hypertension, its cardiovascular aftereffects and lithiasis are also often present in these patients.
3. PLL (posterior longitudinal ligament) may lead to serious repercussions on the spinal cord & root anatomies & functions. Medullary canal stenosis may present with myelopathic features; presenting features are indicative of site of such changes.
Differentiating features between DISH & AS are:
The inflammatory spondyloarthropathies are usually easily distinguishable from non-inflammatory conditions. The clinical history, physical examination, extra-articular features, laboratory results, and various imaging modalities help in reaching the correct diagnosis. Kozanoglu E & colleagues and Moreno AC & colleagues reported Simultaneous occurrence of diffuse idiopathic skeletal hyperostosis and ankylosing spondylitis. However the following features are of importance:
1. HLA B27
2. Spinal fracture is well known in ankylosing spondylitis but exceptional in diffuse idiopathic skeletal hyperostosis (2).
3. SI joint involvement & it’s radiological features are of paramount importance in diagnosis of AS. According to Maertens M et al CT scan is helpful in differentiating the sacroiliitis of spondylarthropathies (6). However Computed tomography of the sacroiliac joints revealed several abnormalities including asymmetric intraarticular partial fusion, osteophytes with or without bridging, and vacuum phenomenon (5). According to Maertens M et al radiological differentiating points are:
a. absence of left side ossified enthesis (it is said that becuaes of presence of big abdominal vessels on left side this side enthesis are not ossified) & osteophytes.
b. The predominantly horizontal nature of the enthesiophyte in DISH.
c. A midthoracic notch was described in DISH which seemed to be confined to noninflammatory conditions, but is not found in ankylosing spondylitis.
Peculiarity of Radiological features of fractures in both AS & DISH (2)
1. Spinal fractures in patients with ankylosing spondylitis or diffuse idiopathic skeletal hyperostosis generally occur spontaneously or after low-energy trauma. Subsequent complications have serious consequences. Late diagnosis either results from missing a radiologically visible fracture or from the presence of an occult "paper thin" fracture.
2. Repeating standard x-rays the second and third weeks and use of a spiral scan or multiple spiral scan could provide early diagnosis.
Physiotherapy in DISH:
Physiotherapy in DISH is individualized according to the presentation. Spinal presentations are treated with mobilization for pain reduction. It must be noted though DISH mostly affects thoracic area, lumbar & cervical area pain may be presented by the patients. Strength training low load high repetition exercises. For acral enthesiopathies electro-therapeutics, soft tissue therapies, mobilization and strengthening can go side by side. Promotion of proper physical activity & modification of stressful ones are also key to successful management. Hydrotherapy is also a useful tool.
References: 1. Reumatismo. 2006 Apr-Jun;58(2):104-11. 2. Rev Chir Orthop Reparatrice Appar Mot. 2004 Sep;90(5):456-65. 3. Rev Rhum Engl Ed. 1996 Apr;63(4):292-5. 4. Clin Rheumatol. 2002 Jun;21(3):258-60. 5. J Rheumatol. 1988 Oct;15(10):1506-11. 6. Clin Rheumatol. 1992 Dec;11(4):551-7. 7. http://www.ima.org.il/imaj/ar03jul-11.pdf.


Comments
Post a Comment