Internal impingement of shoulder: A simple overview
The impingement in shoulder can clearly be classified into internal & external varieties.
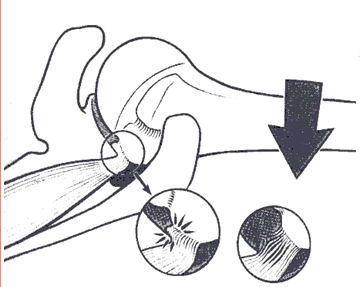
Internal impingement:
The internal impingement syndromes result from the impingement of the soft tissues of the rotator cuff and/or joint capsule on the glenoid or between the glenoid and the humerus.
External impingement:
The external impingement syndromes result from the impingement of the soft tissues of rotator cuff and bursa on the structures of the coracoacromial arch.
External shoulder impingement and rotator cuff disease has been corroborative despite of research arguments. Attempts have been made to identify objective imaging criteria that confirm the diagnosis of impingement, but at present external impingement remains primarily a clinical diagnosis.
Mainly shoulder impingement is caused by compression of the supraspinatus tendon underneath the coracoacromial arch, mostly in forward flexion of the arm.
Stages of external impingement:
Different stages of impingement syndrome are described.
Stage I: There is edema and hemorrhage of the supraspinatus tendon.
Stage II: There is characterized by bursal inflammation and fibrosis, as well as tendinopathy.
Stage III: there is a tear of the rotator cuff.
It is important to remember that clinical signs may overlap in these described stages.
The internal impingement syndrome:
Internal impingement was first described by Walch in 1992 and defined as contact between the supraspinatus tendon and posterior-superior glenoid rim with the shoulder in the cocked, throwing position of 90 degrees of abduction and maximum external rotation.
It is debatable whether internal impingement syndromes truly the result of impingement. Internal impingement seems to be a normal physiological occurrence with the shoulder in certain positions. Imaging findings in internal impingements reveals that these conditions there are 3 different pathologies: undersurface partial-thickness cuff tears, superior labral pathology, and bone changes. According to Paley et al’s study (N=41) in overhead throwing athletes suffering from internal impingement; undersurface cuff fraying was found in 93%, posterosuperior labral fraying was found in 88%, and anterior labral fraying was found in 36% of the subjects.
Theory explaining the internal impingement in overhead athletes:
In athletes where position of extreme abduction and external rotation (ABER position) are repeatedly taken this type of internal impingement occurs. However in simple ABER position also showed physical contact between the undersurface of the rotator cuff and the posterior superior glenoid. In athletes repeated contact between the undersurface of the rotator cuff and the posterosuperior glenoid rim leads to articular-sided partial-thickness rotator cuff tears and superior labral lesions. Hence the "kissing lesions" of undersurface rotator cuff tears and posterosuperior labral damage may be explained by mechanisms other than "internal impingement."
Interestingly Kim et al (2004) have demonstrated flexion as a cause of internal impingement as it affects the labrum. Labral pathologies lead to internal impingement. This study showed that internal impingement in flexion may contribute to the development of Type II SLAP lesions and rotator cuff disease.
Shoulder laxity & instability also has been incriminated as a source of internal impingement but McFarland et al have reported otherwise.
However even the non athletes also suffer from internal impingement. According to McFarland et al contact of the rotator cuff to the posterosuperior glenoid with the arm in abduction and external rotation can occur in a wide spectrum of shoulder disease and is not limited to the throwing athlete.
According to Halbrecht et al internal impingement is also seen in asymptomatic population.
References:
1. Grainger AJ; Semin Musculoskelet Radiol. 2008 Jun;12(2):127-35.
2. Campbell RS et al; Semin Musculoskelet Radiol. 2008 Jun;12(2):107-26.
3. Hodler J; Radiologe. 1996 Dec;36(12):944-50.
4. Budoff JE et al;Arthroscopy. 2003 Oct;19(8):810-4.
5. Kaplan LD et al; Arthroscopy. 2004 Sep;20(7):701-4.
6. Kim TK et al; Clin Orthop Relat Res. 2004 Apr;(421):112-9.
7. McFarland EG et al; J Shoulder Elbow Surg. 1999 Sep-Oct;8(5):458-60.
8. Paley KJ et al; Arthroscopy. 2000 Jan-Feb;16(1):35-40.
9. Halbrecht JL et al; Arthroscopy. 1999 Apr;15(3):253-8.


Comments
Post a Comment